
Should You Withhold Opioids from Patients in Sickle Cell Crisis? The Dogma, The Bias, and What the NCLEX Actually Tests
Sickle cell crisis opioids — and what the NCLEX nursing questions test about them — sit at the intersection of pharmacology, pathophysiology, clinical judgment, and health equity. For patients with sickle cell disease experiencing a vaso-occlusive episode, IV opioids including morphine and hydromorphone are the standard of care for moderate-to-severe pain. Yet these patients are systematically undertreated across emergency departments and wards globally, driven by unsubstantiated concerns about drug-seeking behaviour. The 2020 ASH Guidelines, the 2022 CDC Opioid Prescribing Guideline, and the 2026 NCLEX test plan are aligned: withholding opioids from a patient in sickle cell crisis based on addiction concern is wrong — clinically and ethically.
- Opioids — including IV morphine — are the standard of care for moderate-to-severe vaso-occlusive pain in sickle cell disease. Withholding or delaying opioids based on unsubstantiated drug-seeking concerns is a form of implicit bias that constitutes poor clinical practice and causes measurable patient harm.
- The 2020 ASH Guidelines, the 2022 CDC Opioid Prescribing Guideline (which explicitly excludes SCD from its restrictions), and the 2026 NCLEX test plan are aligned on this.
- On the NCLEX, a nurse who delays opioids for a patient in sickle cell crisis out of addiction concern is choosing the wrong answer.
Why This Is the Most Important Dogma in This Series
Part 1 of this series corrected a pharmacological myth — that morphine worsens pancreatitis. That was a clinical misapplication of incomplete data. This is different.
The underprescription of pain medication to patients with sickle cell disease is not simply a case of outdated science. It is documented, peer-reviewed, racially patterned clinical harm — a form of institutionalised undertreatment that has persisted for decades across emergency departments, wards, and outpatient settings globally.
It kills people. It destroys quality of life. And nurses are directly implicated.
The NCLEX does not test whether you can identify drug-seekers. It tests whether you can provide safe, equitable, evidence-based care. Those are fundamentally different things.
The Classic NCLEX Trap
If you were trained on older materials — or absorbed clinical culture that frames SCD patients as frequent flyers seeking opioids — the following question will reveal that instinct. Recognising it is the first step to answering correctly.
A 28-year-old client with known sickle cell disease presents to the emergency department with a pain rating of 10/10, consistent with previous vaso-occlusive crises. The client requests their usual IV hydromorphone dose. Which action should the nurse take?
Option 1 is correct. ASH 2020 Guidelines recommend analgesic administration within 60 minutes of ED presentation for sickle cell vaso-occlusive pain, with reassessment every 30–60 minutes. The client's request for their known effective analgesic reflects disease-specific pain management history — not drug-seeking behaviour. Option 2 is incorrect — withholding opioids based on drug-seeking suspicion is a form of implicit bias that causes measurable patient harm and has no evidentiary support. Option 3 is inadequate — oral acetaminophen alone is insufficient for acute severe vaso-occlusive pain. Option 4 is incorrect — independently altering a prescribed dose is outside nursing scope of practice and delays adequate analgesia.
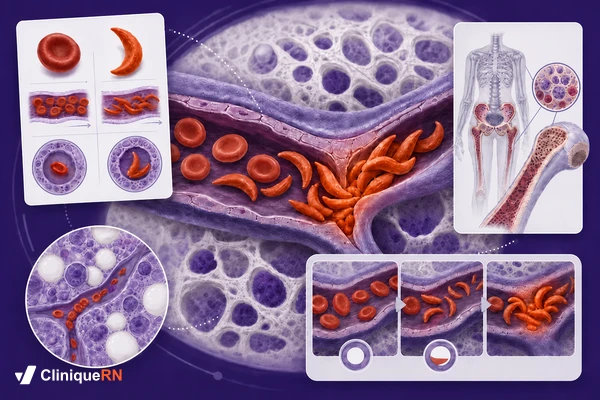
What Happens in a Vaso-Occlusive Crisis
Haemoglobin S polymerises under low oxygen, acidosis, or dehydration — causing red blood cells to sickle and block microvasculature in bone marrow, joints, and lungs. The resulting ischaemic pain is among the most severe a human can experience, and is the primary target of emergency nursing care.
A vaso-occlusive episode (VOE) — also called a sickle cell crisis — occurs when abnormally shaped, rigid haemoglobin S-containing red blood cells aggregate and obstruct microvasculature. The result is tissue ischaemia, infarction, and inflammatory cascade activation — the same mechanisms responsible for ischaemic stroke and myocardial infarction, occurring simultaneously in multiple tissues including bone marrow, joints, lung, spleen, and abdomen.
This is not musculoskeletal soreness. This is not drug-seeking. This is ischaemic tissue death at the microvascular level, producing pain that has been compared by patients and validated by research to be among the most severe pain a human being can experience.
Key Pathophysiology Points the NCLEX May Test
- HbS Polymerisation — Haemoglobin S polymerises under low oxygen tension, acidosis, dehydration, temperature extremes, and physical or emotional stress — triggering the sickling process.
- Shortened RBC Lifespan — Sickled cells are rigid, sticky, and short-lived — 10–20 days versus 120 days for normal RBCs — causing both vascular obstruction and chronic haemolytic anaemia.
- Four Types of Crisis — Vaso-occlusive (most common), hyperhemolytic, splenic sequestration, and aplastic — each with a distinct clinical presentation and nursing priority.
- Major Complications — Acute chest syndrome (ACS), stroke, avascular necrosis, renal failure, and priapism — all potentially triggered or worsened by undertreated vaso-occlusive episodes.

Opioid Bias in Sickle Cell Disease: What the Evidence Shows
Patients with SCD are systematically undertreated for pain despite evidence that opioid addiction rates are approximately 3%. Unsubstantiated drug-seeking concerns — not clinical evidence — drive this undertreatment, causing patients to present to hospital sicker than necessary.
The claim that SCD patients are drug-seeking — repeated in nurse break rooms, embedded in clinical culture, and documented in the peer-reviewed literature as a major source of suboptimal care — has no credible evidentiary foundation.
What the Data Actually Shows
The American Academy of Family Physicians states directly that pain from a vaso-occlusive crisis is often undertreated because of concerns about narcotic addiction and tolerance, perceived drug-seeking behaviour, excessive sedation, respiratory depression, and lack of specific findings on physical examination.
Physicians often fail to prescribe narcotics appropriately and tend to overestimate opioid dependence in patients with pain crises. Yet the incidence of opioid analgesic addiction in patients with sickle cell disease has been reported to be no higher than 3 percent.
American Academy of Family Physicians
Three percent. For a disease where virtually every patient will experience a vaso-occlusive crisis — often dozens of times per year, across a lifetime.
A 2022 systematic review published in Cureus (Arzoun et al.) examining opioid use during VOC found that the available evidence does not support the characterisation of SCD patients as drug-seeking. The pattern of opioid use in SCD patients is driven by disease activity — not behavioural addiction.
A 2024 study in JAMA Internal Medicine (Kang et al.) found that after the 2016 CDC opioid prescribing guideline — which, despite being intended for general chronic pain and not SCD — led clinicians to reduce opioid prescriptions for SCD patients, hospitalisation rates for vaso-occlusive crises increased. When patients cannot manage pain at home due to inadequate prescribing, they present to hospital sicker.
What the Major Guidelines Say About Sickle Cell Pain
ASH 2020 and the 2022 CDC Opioid Guideline — which explicitly excludes sickle cell disease — are aligned: IV opioids are the standard of care for moderate-to-severe vaso-occlusive pain. No guideline recommends withholding opioids pending behaviour assessment.
1. American Society of Hematology (ASH) — 2020 Guidelines
The ASH 2020 Guidelines for Sickle Cell Disease: Management of Acute and Chronic Pain (Blood Advances, 2020; Brandow et al.) are the definitive evidence-based authority on this topic in North America.
On timing: For adults and children with SCD presenting to an acute care setting with acute pain, rapid (≤1 hour of ED arrival) assessment and administration of analgesia with frequent reassessments every 30–60 minutes is recommended (strong recommendation).
On opioid selection: For adults and children with SCD for whom opioid therapy is indicated, tailored opioid dosing based on consideration of baseline opioid therapy and prior effective therapy is suggested.
On interdisciplinary care: Optimal pain management is interdisciplinary. Patient preferences for acute pain management should be incorporated into shared decision-making.
On non-opioid adjuncts: A short course (5–7 days) of NSAIDs in addition to opioids is suggested for acute pain.
There is no recommendation to withhold or delay opioids pending behaviour assessment.
2. CDC Clinical Practice Guideline for Prescribing Opioids — 2022
The 2022 CDC Clinical Practice Guideline for Prescribing Opioids is unambiguous on this point. The American Society of Hematology issued a formal statement welcoming the exclusion. The CDC itself maintains separate guidance documents specifically addressing SCD pain — acknowledging that it requires a distinct, non-restrictive clinical framework.
The recommendations do not apply to pain related to sickle cell disease or cancer, or to patients receiving palliative or end-of-life care. — CDC Clinical Practice Guideline for Prescribing Opioids, 2022 (MMWR)
3. The Structural Racism Dimension
Post-2020 peer-reviewed literature is increasingly direct about what drives SCD undertreatment. A 2024 review states that patients with SCD have long endured structural racism and negative implicit bias surrounding the management of pain, and that it is important to approach the management of inpatient pain systematically with the use of multi-modal medications and nonpharmacological treatments.
The 2026 NCLEX test plan explicitly reflects the NCSBN's integration of health equity principles. Choosing to withhold or delay opioids from a sickle cell disease patient based on assumptions about drug-seeking is a testable, markable wrong answer on the 2026 NCLEX. Safe and Effective Care Environment — Management of Care (17–23%) includes unbiased clinical practice as a tested competency.
Four NCLEX Nursing Priorities in Sickle Cell Crisis
Rapid opioid analgesia within 60 minutes, IV hydration, supplemental oxygen only for documented hypoxia (SpO2 < 95%), and vigilant monitoring for acute chest syndrome and stroke. These four priorities — and their correct sequence — are the core of NCLEX sickle cell disease questions.
Priority 1: Analgesia — Fast and Adequate
ASH recommends analgesic administration within 60 minutes of presentation. IV opioids (morphine, hydromorphone) are standard for moderate-to-severe vaso-occlusive episodes. The patient's prior effective analgesic history should guide dosing — this is individualised care, not a sign of addiction. Reassess pain every 30–60 minutes and titrate accordingly. NSAIDs (short course 5–7 days) can be added as adjuncts.
'Assess pain using a standard scale before administering anything' — this is partially correct but cannot be used to justify significant delay. Assessment and administration should proceed in rapid sequence. Delaying opioid administration while conducting a prolonged assessment, or waiting for physician re-evaluation of drug-seeking before acting on an existing order, is the wrong answer on the NCLEX.
Priority 2: Hydration
IV fluids support haemodilution, reduce sickling, and support renal perfusion. Oral fluids are appropriate for milder presentations; IV access and IV fluids are standard for hospitalised patients. Avoid overhydration in patients at risk for acute chest syndrome, as pulmonary fluid overload can precipitate or worsen ACS.
Priority 3: Oxygenation
Supplemental oxygen is indicated for hypoxic patients (SpO2 < 95%) or those with signs of acute chest syndrome. Routine supplemental oxygen in non-hypoxic SCD patients is not recommended — this is a common NCLEX distractor. Placing a patient in semi-Fowler's to high Fowler's position optimises lung expansion and is appropriate for all hospitalised SCD patients.
Priority 4: Monitor for Life-Threatening Complications
| Complication | Key Signs | Priority Nursing Action |
|---|---|---|
| Acute Chest Syndrome (ACS) | Fever, chest pain, new infiltrate on CXR, hypoxia, tachypnoea | Immediate escalation — apply supplemental O2, notify physician urgently; ACS can be fatal |
| Stroke | Sudden neurological deficit, severe headache, confusion | Emergency CT and neurology consult; activate stroke protocol |
| Splenic Sequestration | Sudden drop in Hgb, rapidly enlarging spleen, hypovolaemia | IV fluids, prepare for transfusion, urgent escalation |
| Aplastic Crisis | Severe anaemia, fatigue, pallour — often follows parvovirus B19 infection | Transfusion support, supportive care, monitor closely |
| Priapism | Painful sustained erection lasting more than 4 hours | Hydration, analgesia, urgent urology consult |
- C — Control pain promptly: IV opioids within 60 minutes; do not delay based on drug-seeking concerns.
- R — Reassess every 30–60 minutes: titrate, document, and communicate response to analgesia.
- I — IV fluids: hydration reduces sickling and supports renal perfusion.
- S — Supplemental O2 only if SpO2 is below 95%: not routine for all patients in crisis.
- I — Individualise dosing: prior effective therapy guides the current analgesic plan.
- S — Screen for complications: ACS, stroke, splenic sequestration, and aplastic crisis.

The 2026 NCLEX and Health Equity: Sickle Cell Disease
Under the 2026 NCLEX-RN test plan, health equity is integrated across all client needs categories — a nurse who delays opioids based on drug-seeking assumptions is choosing the wrong answer. The CJMM consistently identifies prompt analgesia, hydration, and complication monitoring as the correct priority actions.
NCLEX Test Plan Alignment
Under the 2026 NCSBN NCLEX-RN Test Plan (effective April 1, 2026), this topic spans multiple high-weight categories:
| NCLEX Category | Weight |
|---|---|
| Physiological Integrity — Basic Care and Comfort | 6–12% |
| Physiological Integrity — Pharmacological and Parenteral Therapies | 13–19% |
| Physiological Integrity — Physiological Adaptation | 11–17% |
| Safe and Effective Care Environment — Management of Care | 17–23% |
Clinical Judgment Measurement Model (CJMM) Applied
| CJMM Step | Application to SCD Crisis Scenario |
|---|---|
| 1. Recognise Cues | Patient with known SCD, pain 10/10, prior history of VOE, requests usual opioid dose |
| 2. Analyse Cues | Is there a clinical reason to withhold? Is this consistent with prior crises? (Answer: No clinical reason to withhold) |
| 3. Prioritise Hypotheses | VOE is most likely; priority is pain control and complication prevention |
| 4. Generate Solutions | Administer IV opioid per order; reassess in 30 minutes; assess for ACS, initiate hydration |
| 5. Take Action | Give the medication. Assess pain response. Initiate hydration. Monitor SpO2. |
| 6. Evaluate Outcomes | Is pain controlled? Are there signs of ACS, stroke, or sequestration? |
CliniqueRN Practice Questions
A client with sickle cell disease arrives at the ED with pain rated 10/10, consistent with their previous vaso-occlusive crises. The client states: 'I need my usual dose of IV hydromorphone — nothing else works.' The triage nurse says to you: 'This client is here every month. I think they just want opioids.' Which nursing action is the priority?
Option 3 is correct. The ASH 2020 Guidelines recommend analgesic administration within 60 minutes of ED presentation for SCD-related pain. The client's request for their known effective analgesic reflects disease-specific pain management history — not drug-seeking behaviour. The incidence of opioid addiction in SCD patients is documented at approximately 3%, yet these patients are systematically undertreated due to unsubstantiated clinical bias. Option 1 delays treatment inappropriately — the nurse's role is to advocate for the patient and implement the care plan, not to deliberate with colleagues about whether the patient deserves opioids. Option 2 is inadequate — oral acetaminophen alone is insufficient for acute severe vaso-occlusive pain. Option 4 constitutes an independent alteration of a physician order, which is outside nursing scope of practice and delays adequate analgesia. When the NCLEX presents another nurse expressing suspicion about a SCD patient's pain, treat that as a distractor introducing bias — not clinical evidence.
A nurse is caring for a hospitalised client with sickle cell disease on day 2 of a vaso-occlusive crisis. The client's pain is currently 5/10 on IV morphine scheduled every 4 hours. The client suddenly develops a fever of 38.9°C (102°F), begins reporting chest pain rated 7/10, and their oxygen saturation drops from 97% to 91% on room air. Which action should the nurse take FIRST?
Option 2 is correct. The triad of fever, chest pain, and hypoxia — SpO2 dropping to 91% — in a patient with SCD is the classic presentation of Acute Chest Syndrome (ACS), one of the most life-threatening complications of sickle cell disease and a leading cause of SCD-related mortality. ACS is defined as a new pulmonary infiltrate on CXR accompanied by fever and respiratory symptoms. The nurse's immediate priority is oxygenation support — supplemental O2 for SpO2 below 95% — and urgent physician notification. Option 1 addresses pain but misses the priority emergency; ACS takes precedence. Option 3 delays critical intervention — the physician must be notified immediately, not after awaiting radiology results. Option 4 is dangerous — dismissing FEVER + CHEST PAIN + HYPOXIA as routine vaso-occlusive pain could result in patient death. In SCD questions, when you see this triad together, think Acute Chest Syndrome — not just VOE.
A nurse is preparing discharge teaching for a client with sickle cell disease following a vaso-occlusive crisis admission. Which statement by the client indicates a need for further teaching?
Option 3 indicates a need for further teaching. Routine supplemental oxygen between crises in non-hypoxic SCD patients is not recommended. Home oxygen is only indicated for documented hypoxia (SpO2 below 95%) or specific complications such as ACS. The statement that supplemental oxygen at home between crises prevents sickling is factually incorrect and provides false reassurance. Options 1, 2, and 4 all reflect accurate and important self-management teaching. Staying well hydrated is the most evidence-based preventive strategy patients can control. Recognising escalation cues — fever, inability to manage pain at home — and knowing triggers are both appropriate teaching points. Additional NCLEX-testable triggers for vaso-occlusive crisis include: dehydration, infection, cold exposure, hypoxia, high altitude, strenuous physical activity, psychological stress, and alcohol use.
A 35-year-old client with sickle cell disease is admitted for a vaso-occlusive crisis. Current assessment: pain 9/10, HR 112, BP 138/88, RR 20, SpO2 97%, temperature 37.2°C. The client reports the pain is identical to previous crises and that IV morphine is the only thing that works. The physician orders IV morphine 4 mg every 3 hours PRN, IV normal saline at 125 mL/hr, and acetaminophen 1,000 mg PO every 8 hours. Select ALL nursing actions that are appropriate at this time.
Options 1, 3, 4, and 6 are correct. Option 1 is correct — IV morphine should be administered promptly per the physician order; ASH 2020 guidelines support opioid analgesia for acute SCD pain. Option 2 is incorrect — there is no clinical or guideline basis for withholding opioids pending an addiction consult in acute VOE; this causes harm and reflects implicit bias. Option 3 is correct — acetaminophen as a scheduled non-opioid adjunct is supported by ASH 2020 guidelines as part of multimodal pain management. Option 4 is correct — IV hydration is standard supportive care for VOE, reducing blood viscosity and supporting sickling reversal. Option 5 is incorrect — the client's SpO2 is 97%; supplemental oxygen is not indicated in a non-hypoxic patient and is not routine for all SCD crises per current guidelines. Option 6 is correct — reassessment within 30–60 minutes is recommended by ASH to evaluate analgesic effect and adjust the care plan. Option 7 is incorrect — opioids are the current standard of care for moderate-to-severe acute SCD pain; this statement is factually wrong and potentially harmful to the client.
The Evidence Hierarchy — At a Glance
| Claim | Source | Verdict |
|---|---|---|
| Opioids are standard for moderate-to-severe VOE | ASH 2020 Guidelines, Blood Advances | Supported |
| Analgesics should be given within 60 minutes of presentation | ASH 2020 Guidelines | Supported |
| SCD is excluded from CDC opioid restrictions | CDC 2022 Opioid Guideline, MMWR | Confirmed |
| Opioid addiction rate in SCD is approximately 3% | AAFP; multiple peer-reviewed reviews | Supported |
| Supplemental O2 is routine for all SCD crises | Not supported by any current guideline | Myth |
| SCD patients frequently exhibit drug-seeking behaviour | No credible clinical evidence base | Myth / Documented Bias |
| Underprescribing opioids for SCD causes harm | Kang et al., JAMA Internal Medicine 2024 | Confirmed |
Sickle Cell Crisis Opioids NCLEX — Key Takeaways
- IV opioids (morphine, hydromorphone) are the standard of care for moderate-to-severe vaso-occlusive pain — confirmed by ASH 2020 Guidelines
- Analgesics must be administered within 60 minutes of ED presentation, with reassessment every 30–60 minutes
- Sickle cell disease is explicitly excluded from the 2022 CDC Opioid Prescribing Guideline restrictions
- The incidence of opioid addiction in SCD patients is approximately 3% — yet these patients are systematically undertreated due to unsubstantiated clinical bias
- Routine supplemental oxygen is NOT recommended for all SCD crisis patients — only for SpO2 below 95%
- Use the CRISIS mnemonic: Control pain, Reassess frequently, IV fluids, Supplemental O2 only if needed, Individualise dosing, Screen for complications
- ACS (fever + chest pain + hypoxia) is a nursing emergency requiring immediate escalation — not reassurance
- On the 2026 NCLEX, withholding opioids from a SCD patient based on drug-seeking concerns is a markable wrong answer — it reflects implicit bias, not evidence-based clinical judgment
Frequently Asked Questions
Are opioids appropriate for vaso-occlusive crisis pain in sickle cell disease?
What does the ASH 2020 guideline recommend for sickle cell pain management?
Does the CDC opioid prescribing guideline restrict treatment for sickle cell disease?
What is acute chest syndrome and how should a nurse respond?
Should all patients in sickle cell crisis receive supplemental oxygen?
Why are sickle cell disease patients often undertreated for pain?
Sources and References
- Brandow AM, Carroll CP, Creary S, et al. American Society of Hematology 2020 Guidelines for Sickle Cell Disease: Management of Acute and Chronic Pain. Blood Advances. 2020;4(12):2656–2701. DOI: 10.1182/bloodadvances.2020001851
- Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC Clinical Practice Guideline for Prescribing Opioids for Pain — United States, 2022. MMWR Recomm Rep. 2022;71(3):1–95.
- CDC. Healthcare Providers: Managing Sickle Cell Disease Pain. Centers for Disease Control and Prevention. cdc.gov/overdose-prevention.
- American Society of Hematology. ASH Statement on New Opioid Prescribing Guidelines. 2022. hematology.org/newsroom/press-releases/2022
- Kang HA, Wang B, Barner JC, et al. Opioid Prescribing and Outcomes in Patients With Sickle Cell Disease Post-2016 CDC Guideline. JAMA Internal Medicine. 2024;184(5):510–518.
- American Academy of Family Physicians. Approach to the Vaso-occlusive Crisis in Adults with Sickle Cell Disease. Am Fam Physician. 2000;61(5):1349–1356.
- Arzoun H, Srinivasan M, Sahib I, et al. Opioid Use in Patients With Sickle Cell Disease During a Vaso-Occlusive Crisis. Cureus. 2022;14(1):e21473.
- National Academies of Sciences, Engineering, and Medicine. Chapter 3: Pain Management in Sickle Cell Disease. 2025.
- Inpatient Management of Pain Episodes in Children with Sickle Cell Disease: A Review. MDPI. 2024. PMC11430294.
- NCSBN. 2026 NCLEX-RN Test Plan. National Council of State Boards of Nursing. Effective April 1, 2026. ncsbn.org/publications/2026-nclex-rn-test-plan.
- StatPearls. Sickle Cell Anemia (Nursing). NCBI Bookshelf. Updated 2023. Available at: ncbi.nlm.nih.gov/books
Practice Sickle Cell Disease and High-Yield NCLEX Pharmacology Questions on CliniqueRN
Start Free PracticeKeep Reading
- Is Morphine Contraindicated in Pancreatitis? What the NCLEX Tests vs. What Evidence Says
- MONA Mnemonic Obsolete for ACS: 2025 AHA/ACC Guidelines & the NCLEX
- STOP Guessing on SATA! This Strategy Is the Game-Changer You Need
- 7 Uncommon NCLEX Study Tactics That Actually Work
- NCLEX Cardiac Nursing Essentials: Heart Conditions, Meds & Priority Interventions